

Speciality
ORTHOPTICS
- Orthoptics work with patients of all ages children to the elderly.
- To investigate, diagnose and treat side related problems and abnormalities of eye movements and eye position.
ANATOMY AND PHYSIOLOGY OF THE OCULAR MOTILITY SYSTEM
- EXTRA OCULAR MUSCLES
- OCULAR MOTILITY
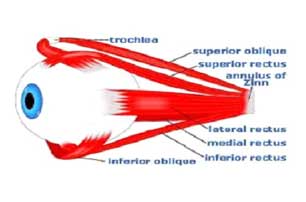
- EXTRA OCULAR MUSCLES
There are 4 Rectus and 2 Oblique Muscle.
The primary function of 4 Rectus muscles is to control the eyes movements from left to right and up and down.
The two oblique muscles rotate the eyes inward and outward.
Top
FOUR RECTUS MUSCLES ARE:
- Superior Rectus (SR)
- Inferior Rectus IR)
- Medial Rectus (MR)
- Lateral Rectus (LR)
TWO OBLIQUE MUSCLES ARE:
- Medial Oblique (MO)
- Inferior Oblique (IO)
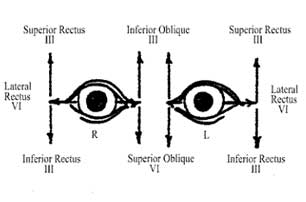
NERVE SUPPLY TO THE EYE:
- The Extra Ocular Muscles are innervated by Third, Fourth & Sixth Cranial nerve.
- The upper division of the Occulomotor nerve (3rd Cranial nerve) innervates the The Superior Rectus.
- The lower division of Occulomotor nerve innervates the Inferior Rectus,Medial Rectus and Inferior Oblique muscles.
- The Trochlear nerve (4th Cranial Nerve) Innervates the Superior Oblique muscle.
- The Abducens Nerve ( 6th Cranial nerve) Innervates the Lateral Rectus Muscle.
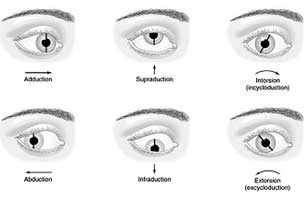
OCULAR MOVEMENTS
- Duction : Monocular movement are called Duction.
- Adduction : Movement of the eye towards the nose.
- Abduction : Movement of the eye away from the nose.
- Elevation : Movemet of the eye Upward.
- Depression : Movement of the eye Downward.
- Extortion : Movement of the eye away from the nose in upward motion.
- Intortion : Movement of the eye towards the nose in upward motion.
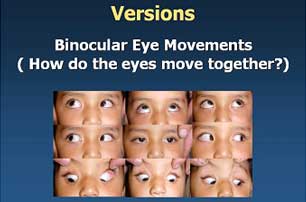
OCULAR MOVEMENTS
These are of two types: Versions and Vergennce- Versions : Movement of the eye in the same direction also known as conjugate movements.
- Dextroversins : It is the Movement of both eyes to the right.
- Levoversions : It is the movement of both eyes to the left.
- Supraversion : It is upward movement of both eyes in primary position of eye.
- Ifraversion : It is downward movement of both eyes in primary position of eye.
- Dextrocycloversion : In this Superior pole of Cornea of both eyes tilts towards the right.
- Levocycloversion: In it Superior pole of cornea of both eyes tilts towards the left.
- Vergence : Symmetric movements of both eyes in opposite direction also called as disjugate movement.
- Convergence : It is simultaneous inward movement of both eyes.
- Divegence : It is simultaneous outward movement of both eyes.
Top
EXTRA OCULAR MUSCLES AND ACTION
| MUSCLE NAME | ACTION |
| Medial Rectus | Adduction |
| Lateral Rectus | Abduction |
| Inferior Rectus Extorsion Adduction | Depression |
| Superior Rectus Intorsion Adduction | Elevation |
| Superior Oblique Depression Abduction | Intorsion |
| Inferior Oblique Elevation Abduction | Extortion |
BINOCULAR SINGLE VISION
- What Is Binocular Single Vision?
- PREREQUISITES FOR DEVELOPMENT OF BINOCULAR SINGLE VISION
- Straight Eye
- Reasonable clear vision
- Ability of Visual Axis
- GRADES OF BINOCULAR SINGLE VISION
When the normal Individual looks at the object ,the image is formed on the both eyes saperately; but the individual can see a single image. This state is called as Binocular Single vision.
Grade 1: Simultaneous Perception
It is the power to see two dissimilar objects simultaneously. For Example- When the picture of a bird is projected onto the right eye and that of a cage onto the left eye, an Individual with presence of Simultaneous Perception will see the bird in the cage.
Grade 2 :Fusion
It consist of the power to Superimpose two incomplete but similar image to form one complete image.
Grade 3 : Stereopsis
It consist of the ability to see the third dimension(Depth Perception).
ANOMALIES OF BINOCULAR VISION
Anomalies of binocular vision include:- Amblyopia
- Diplopia
- Supression
- Abnormal Retinal Correspondence (ARC)
- Strabismus (Squint)
AMBLYOPIA
Amblyopia is the clinical term for lazy eye. An Amblyopic eye is normal structure wise,but vision is poor.TYPES OF AMBLYOPIA
- Anisopmetropic Amblyopia: It is caused due to large difference in refractive error between both the eyes.
- Ametropic Amblyopia: It is caused due to high refractive error in both eyes. Hyperopia has a greater chance causing Amblyopia when compared to myopia.
- Stimulus deprivation Amblyopia: It is caused due to media opacities which prevent the clear image to be formed on the retina.
- Strabismic Amblyopia: It is caused due to Misalignment of Visual Axis early in the age.
Amblyopia develops between birth and 7 to 8 years of age, the critical period when the eye is in the process of development.
It must be indentified and treated before the child becomes 7 or 8 years old, otherwise the vision loss becomes irreversible.
Top
Treatment
- Cycloplegic Refraction & full correction of Refractive Error
- Removing the cause of stimulus Deprivation
- Correction of Squint
- Patching of the good eye
- Pharmalogical Penalization of the non- Amblyopic eye using Atropine eye drop.

DIPLOPIA
Perceiving double image of an object is called as Diplopia. It occurs even when the normal eye is closed(Uniocular Diplopia) or only When both eyes are open (Binocular Diplopia).
COMMON CAUSES OF DIPLOPIA:
- Uniocular Diplopia
- SubLuxated Diplopia
- Double pupil
- Incipient Cataract
- Keratoconus
- Binocular Diplopia
- Paralytic Squint
- Myasthania Gravis
- Diabetes
- Thyroid Disorder
- Anisometropic Glasses (e.g. Uniocular Aphakik Glasses)
- After Squint correction in the presence of abnormal retinal correspondence.
SUPPRESSION
It is a temporary active cortical inhibition of the image of an object formed on the retina of the Squinting eye.This phenomenon occurs only during binocular vision when both eyes are open.
However,when the fixating eye is covered , the squiting eye fixes.
TEST TO DETECT SUPPRESSION
- Worths 4-dots test
- Four diopter base out prism test
- Red glass test
- Synoptophore test
ABNORMAL RETINAL CORRESPONDOUS (ARC)
The fovea of two eyes acts as corresponding points and have the same visual direction this is called as Normal Retinal Correspondence. When Squint develops, patient experience either Diplopia or Confusion. To Avoid these, sometimes there occurs an active cortical adjustment in the directional values of the two retinae In this state fovea of the normal eye and an extrafoveal point on the retina of the squinting eye aquire a common visual direction. This condition is called as Abnormal Retinal Correspondous.TEST TO DETECT ABNORMAL RETINAL CORRESPONDENCE
- Worths 4-dots test
- Titmus Stereotest
- Bagolini Straight glass test
- After image test
- Synoptophore test
STRABISMUS
Normally Visual axis of the two eyes are parrellel to each other in the primary position of gaze and this alignment is maintained in all position. A misalignment of the Visual Axis of two eyes is called Squint or Strabismus.- STRABISMUS IS CLASSIFIED AS
- Hetrophoria
- Hetrotropia
HETROPHORIA
Hetrophoria is the Latent Squint.Patients eye will not show deviation it looks straight. In this condition the tendency of the eye to deviate is kept latent by fusion. Therefore when the fusion is removed the visual axis of one eye deviates away.
Top
TYPES OF HETROPHORIA
- Esophoria:-It is a tendency of eye to move towards the nose that is to converge.
- Exophoria:- It is a tendency of eye to move outwards towards the temple that is to diverge.
- Hyperphoria:- It is a tendency to move the eye upwards.
- Hypophoria:- It is a tendency of eye to move downwards.
HETROTROPIA
Hetrotropia is the Menifest Squint. We can see the deviation in the patients eye it wont be straight.
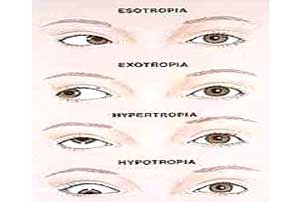
TYPES OF HETROTROPIA
- Exotropia: deviation of eye towards the temporal side.
- Esotropia: Deviation of eye towards the nasal side.
- Hypertropia: Deviation of eye in the Upward direction.
- Hypotropia: Deviation of eye in the Downward direction.
Top
Also Visit


News & Events
Akshar eye clinic proudly acounces the addition of new machine that is Zeiss FDT( Frequency doubling technolgy )Perimetry. The instrument is designed for fast and effective detection of visual loss. Which one of the few ophthalmologist have.

Seasonal Disease
Allergic conjunctivitis or spring catarrh is a very common seasonal disorder in children between 5 - 15 years of age. The disorder can only be suppressed. Cure cannot be offered.
Download Brochure

